Molly – 2 year old Labrador with a Torn ACL
After playing at a park, 2 year old Labrador Molly was diagnosed with a torn ACL (or anterior cruciate ligament) by another veterinary clinic. After presenting at BPS, an exam confirmed that an ACL tear had occurred and further testing revealed a significant anterior draw sign (the ability to move the tibia forward in comparison to the femur). We also assessed Molly’s hip, hock and achilles but these areas were determined to be okay.
These sorts of cases are rarely x-rayed, as a clinical exam is usually sufficient to diagnose these sorts of injuries and an x-ray won’t offer any new information. Rather, it will just cost the owner money that could otherwise be spent on surgery or treatment.
A week later, Molly was admitted to our veterinary hospital to have her ACL repaired using a process known as Zlig.
After being admitted for LH ACL stabilisation using Zlig, Molly was first placed onto IV fluids via catheter (290ml per hour) pre induction. She was also intubated, placed onto 02/ISO gas and given atropine via IV. Post induction, Molly was given an IV containing betamox, metacam sc, keflin and fentanyl. She also had a fentanyl patch applied and was placed onto a fentanyl infusion.
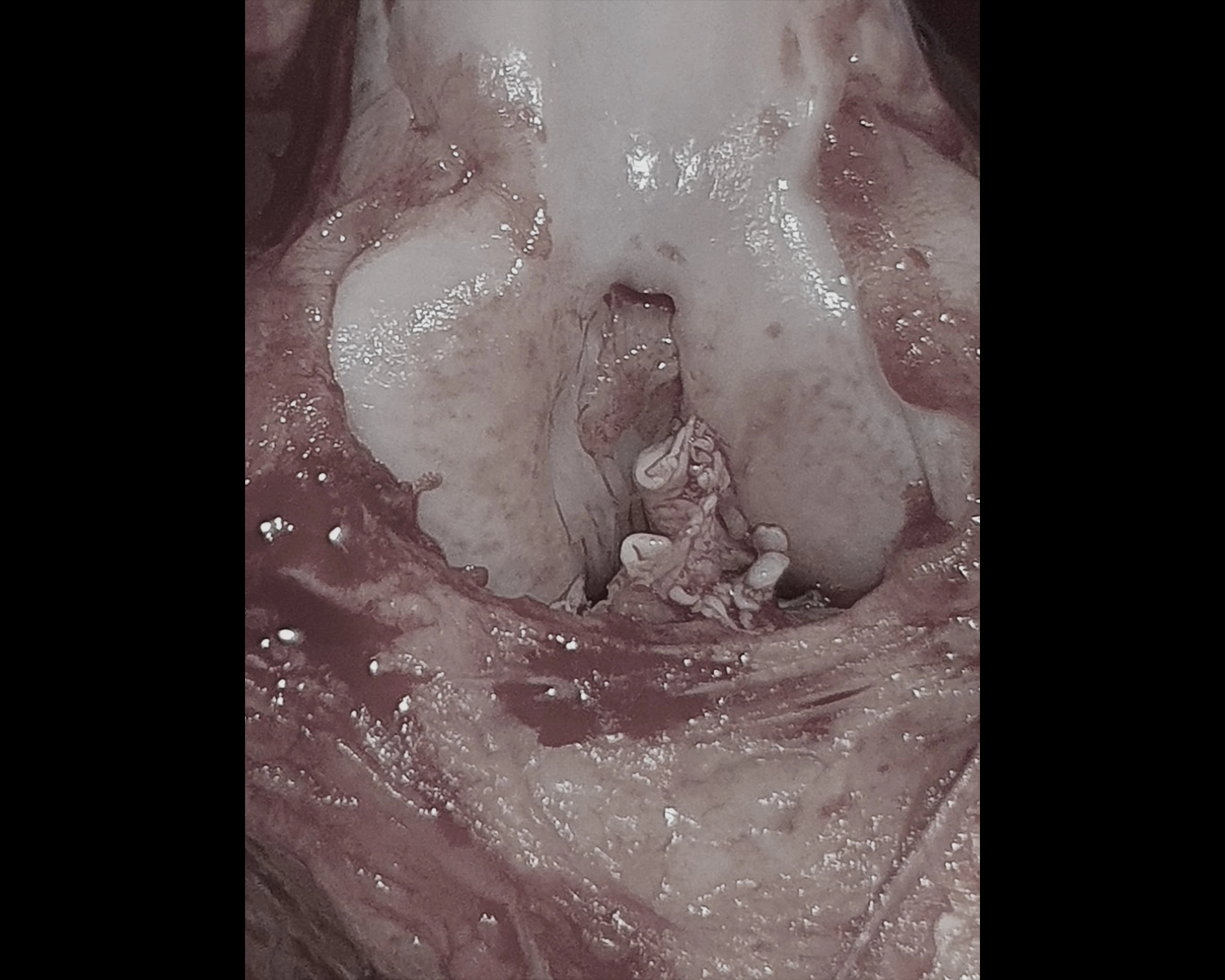
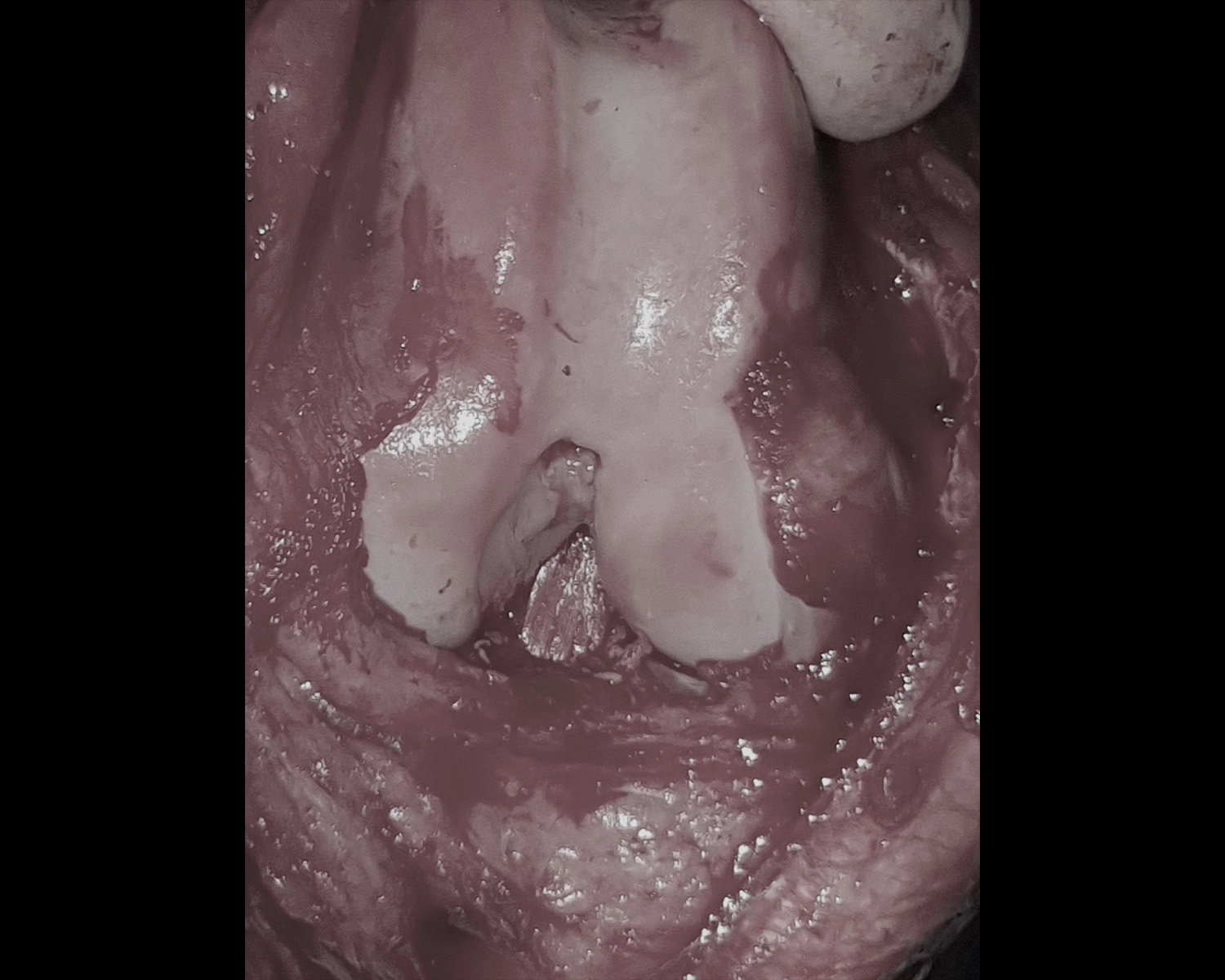
Once surgery commenced, the skin over Molly’s medial LH stile was cut open. A medial arthrotomy was performed and the patella was laterally reflected. We were able to identify the remnants of the torn ACL and removed, then a pin was placed through the medial wall of the distal femur’s lateral wall. We used a cannulated drill to drive through the femoral condyle, then a pin was placed into the insertion point of the tibia which passed out through the tibial crest further down. Finally, a 25 to 45kg 19mm Zlig implant was inserted through the tibia and joint before being passed out through the femur and a cannulated screw placed in the exit.
We checked the stifle for normal movement, clamped the implant at the exit from the tibial crest, and checked the anterior draw sign (which was no longer present). After the cannulated screw was placed in the tibial crest, a hole was drilled into the femur (around 1.5cm from the condyle exit) and implants were passed through (from lateral to medial). The ligament was then trimmed over the medial distal femur (at the lateral exit from the tibia).
Procedure photos for recent case